

The finding of biological markers of specific language impairment would facilitate their detection and early intervention. In this sense, the 2D:4D finger ratio is considered an indirect indicator of prenatal exposure to testosterone. Previous studies have related it to linguistic competence and aggressive behaviour, and could be a candidate for a biological marker of language impairment. The aim was to compare the value of the 2D:4D ratio in children with Specific Language Impairment (SLI) with those of children with typical language development, as well as to establish to what extent this biological index correlates with the behaviour (linguistic, cognitive, social,...) in both groups.
Subjects and methods2D:4D ratio, language, cognition and social behaviour were compared in a group of children with SLI (n=15), with a group of children without language difficulties (n=16) of the same age (between 5 and 8 years), gender (male), and socio-cultural level.
ResultsChildren with SLI showed significantly higher values of 2D:4D ratio of the right hand, and a negative correlation between this ratio and their linguistic competence. Although the children with SLI showed impaired adaptive abilities, but not more aggressive behaviour, these measurements did not correlate with the 2D:4D index. Nevertheless, social behaviour correlated with language and cognition competence.
ConclusionsA higher value of the biological 2D:4D ration (lower intrauterine exposure to testosterone) seems to be associated with language difficulties in boys with SLI, but not with their behavioural difficulties. Their behavioural difficulties seem to be a consequence of their linguistic difficulties and their level of cognition.
Encontrar marcadores biológicos del trastorno específico del lenguaje facilitaría su detección e intervención precoz. En este sentido, el índice digital D2:D4 es considerado un indicador indirecto de la exposición prenatal a la testosterona, y estudios previos lo han relacionado con la competencia lingüística y la conducta agresiva, por lo que podría ser un candidato a marcador biológico. El objetivo es comparar el valour de este índice digital en niños con trastorno específico del lenguaje (TEL) frente a sujetos con desarrollo típico del lenguaje, estableciendo en qué medida correlacionan los valores del índice biológico con la conducta (lingüística, cognitiva, social…) de dichos sujetos.
Sujetos y métodosSe comparó el índice D2:D4, el lenguaje, la cognición y la conducta social en un grupo de niños con TEL (n=15) con un grupo de niños sin dificultades del lenguaje (n=16) de la misma la misma edad (entre 5–8 años), sexo (masculino) y nivel sociocultural.
ResultadosLos niños con TEL mostraron valores significativamente más altos en el índice D2:D4 de la mano derecha, y una correlación negativa entre el índice D2:D4 de la mano derecha y la competencia lingüística. Aunque los niños con TEL mostraron peores habilidades adaptativas y conductas internalizantes, aunque no mayor agresividad, estas medidas no se correlacionaron con el índice D2:D4, y sí con los valores de lenguaje y de cognición.
ConclusionesUn valour más alto del índice biológico D2:D4 (menor exposición intrauterina a la testosterona) parece estar asociado con las dificultades del lenguaje de los niños con TEL, pero no con sus dificultades conductuales. Las dificultades conductuales de estos niños parecen ser consecuencia de sus dificultades lingüísticas y de su nivel de cognición.
The 2D:4D digit ratio is the quotient between the length of the forefinger and the ring finger and an indirect marker of androgenization in the first trimester of gestation. A lower 2D:4D ratio reflects prenatal exposure to higher levels of testosterone, which results in a low ratio in boys and a high ratio in girls.1 Several studies have demonstrated an association between prenatal testosterone levels and the development of the cerebral hemispheres, inducing the maturation of the right hemisphere or the acceleration of programmed cell death in the left hemisphere.2 These asymmetries in cerebral structure affect various cognitive functions, including language.3 Thus, several studies have demonstrated the important role of testosterone and other prenatal hormones in the presence of sexual dimorphism in the development of spatial skills4 and language,5 especially in the areas of vocabulary and fluency.6
Taking into consideration this association between prenatal androgenization and language development, Geschwind and Galaburda7 hypothesized that an increased prenatal exposure to testosterone would be associated with a higher incidence of language and learning disorders in male compared to female individuals.8 Although several studies support this hypothesis,9,10 the findings of other studies contradict it, both in individuals with and without disorders.7,11–13 Furthermore, the studies that have found evidence of this association could not firmly establish the direction of the effect, that is, whether language problems are associated with a higher or a lower 2D:4D digit ratio, in either the general or the clinical population.14
The contradictory findings of previous studies call for the continued investigation of the association between the degree of androgenization and different language problems as well as the role of nonverbal intelligence in this association. In this sense, it would be key to study this ratio in relation to specific language impairment (SLI), as affected individuals have language problems in the absence of other developmental impairment.15 Furthermore, we know of no studies on this subject in individuals with SLI, and establishing an association between the 2D:4D ratio and SLI would provide a useful biological marker that would contribute to the early diagnosis and treatment of SLI.
Children with SLI have language difficulties in the absence of the causes that usually explain these problems, such as intellectual disability, brain damage, hearing problems or socioemotional problems.15 Their language is mainly characterized by impairments in morphology and syntax, although they may also present problems in expressive vocabulary and speech.16 Neuroimaging studies of individuals with SLI have shown deviation from the normal pattern of volumetric asymmetry of the cerebral hemispheres17 that could be explained by prenatal exposure to high levels of testosterone.3,18,19
In addition, several studies have found an association between SLI and various behavioural disorders,20–22 and it is known that prenatal androgenization increases aggressive behaviour in every species in which this association has been studied, including primates.23 Thus, in children with SLI, increased prenatal exposure could explain the language impairment as well as behavioural problems, which would result from the increase in aggression.
With the ultimate aim of identifying a biological marker of SLI and with the hypothesis that there is a correlation between the 2D:4D digit ratio and language development and adaptive behaviour, we conducted a study with the following objectives: a) to compare the 2D:4D digit ratios in children with SLI versus children with normal language development, b) to describe the behavioural problems associated with the presence of language impairment, and c) to analyze the correlation between the 2D:4D digit ratio and aggressive behaviours in children with SLI.
Participants and methodsParticipantsThe sample consisted of 33 participants, all of them boys aged 5–8 years, divided into 2 groups. The case group initially included 17 boys with SLI (specific language impairment or language disorder based on the DSM-5 criteria), but 2 of them had to be excluded a posteriori, one due to the presence of epileptiform discharges in a subsequent electroencephalogram, and the other for scoring at the 13th percentile in Raven's test, since one of the exclusion criteria for diagnosis of SLI is. The mean age of the cases was 6.19 years. All were bilingual speakers of Catalan and Spanish and resided in Majorca (Balearic Islands). The control group consisted of 16 boys residing in the same island, also bilingual, of a similar socioeconomic level and with a similar body mass index. The mean age in the control group was 6.69 years.
To verify that the diagnostic criteria of SLI were met, we assessed all children in the sample with the Clinical Evaluation of Language Fundamentals-4, Spanish Edition (CELF-4)24 and nonverbal intelligence with the Raven Coloured Progressive Matrices test.25 When it came to hearing, all the cases had verified hearing thresholds of less than 30dB and normal results in the neonatal hearing screening (otoacoustic emissions test). Furthermore, 23 of them had good scores in the screening test performed by the Department of Education at age 6 years, and the other 8 had undergone evaluation by medical providers with no evidence of hearing loss. None of the participants had received a diagnosis of a genetic disorder with or without endocrinological involvement by the paediatric neurology department.
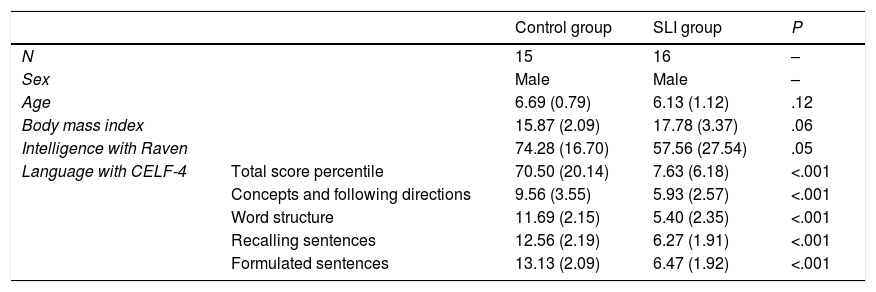
We assessed body mass index, age and intellectual quotient as potential confounding variables, and found no significant differences between the 2 groups in any of them. Table 1 presents the general characteristics of the children included in the sample.
Characteristics of the sample.
| Control group | SLI group | P | ||
|---|---|---|---|---|
| N | 15 | 16 | – | |
| Sex | Male | Male | – | |
| Age | 6.69 (0.79) | 6.13 (1.12) | .12 | |
| Body mass index | 15.87 (2.09) | 17.78 (3.37) | .06 | |
| Intelligence with Raven | 74.28 (16.70) | 57.56 (27.54) | .05 | |
| Language with CELF-4 | Total score percentile | 70.50 (20.14) | 7.63 (6.18) | <.001 |
| Concepts and following directions | 9.56 (3.55) | 5.93 (2.57) | <.001 | |
| Word structure | 11.69 (2.15) | 5.40 (2.35) | <.001 | |
| Recalling sentences | 12.56 (2.19) | 6.27 (1.91) | <.001 | |
| Formulated sentences | 13.13 (2.09) | 6.47 (1.92) | <.001 |
Mean values presented with the standard deviation in parentheses.
Before starting the study, we obtained the informed consent of the parents of every child for their participation. The research protocol was approved by the Research Ethics Committee of the Autonomous Community of Balearic Islands (the CEI-IB) under file name IB 2568/15 PI.
MaterialsWe assessed language using the language subtests in the CELF-4: concepts and following directions, word structure, recalling sentences and formulated sentences.
To assess aggression, we used the Spanish version27 of the Behaviour Assessment System for Children (BASC).26 This multidimensional test measures various aspects of behaviour and personality. In our study, we used the BASC P1 or BASC P2 scale (questionnaires for parents) based on the age of the participant (P1 for participants aged less than 6 years and P2 for those age more than 6 years), which measure maladaptive behaviours (clinical scales: aggression, hyperactivity, conduct problems, attention problems, learning problems, atypicality, depression, anxiety, withdrawal and somatization), and positive behaviours (adaptive scales: adaptability, social skills, leadership and study skills). The test allows the evaluation of 5 composite measures: externalizing problems, internalizing problems, school problems, adaptive skills and a behavioural symptoms index.
For the purpose of calculating the 2D:4D digit ratio, we scanned the hands of participants with a HP LaserJet Pro MFP M125nw scanner at a resolution of 200 dpi.
ProcedureA licensed speech therapist performed all the evaluations. The CELF-4 and the Raven test were scored as specified in their respective manuals, and the raw scores were transformed to percentiles. The BASC P1 and P2 scales were scored using the web-based tool provided by TEA Ediciones. This tool was also used to calculate reliability, validity and consistency indices for the BASC scale for each participant, and only the responses that met the established quality standards were included in the analysis.
The same scanner was used to measure the fingers of all participants, and each hand was scanned twice, always including the same grid in one of the corners of the scanner bed to ensure that the same scale was applied in every measurement. Each child was asked to press the palms of both hands against the glass of the scanner bed with the fingers fully extended and spread out to obtain a sharp image of the boundaries of each phalanx. Once the scanned image was obtained and saved in jpg format, it was opened in Adobe Photoshop to measure the length of the second and the fourth fingers of each hand from the midpoint of the bottom crease of the finger to the midpoint of the distal tip. Two individuals independently measured each of the fingers in each hand (the first author of the article and an individual not involved in the study who was familiar with the software), and we calculated the mean of the 2 measurements for each finger. We used these mean values to calculate the ratio of the length of the index finger (2D) and the ring finger (4D) in each hand.
We used these values to calculate the mean and standard deviation for each group for each of the measurements. In the comparative analysis, we assessed normality with the Shapiro–Wilk, and used the Student t test to compare variables with a normal distribution and the Wilcoxon test otherwise. We used the Pearson correlation coefficient to analyze the association between the 2D:4D digit ratio and different behavioural variables. We defined statistical significance as a p-value of less than 0.05 in any of the tests.
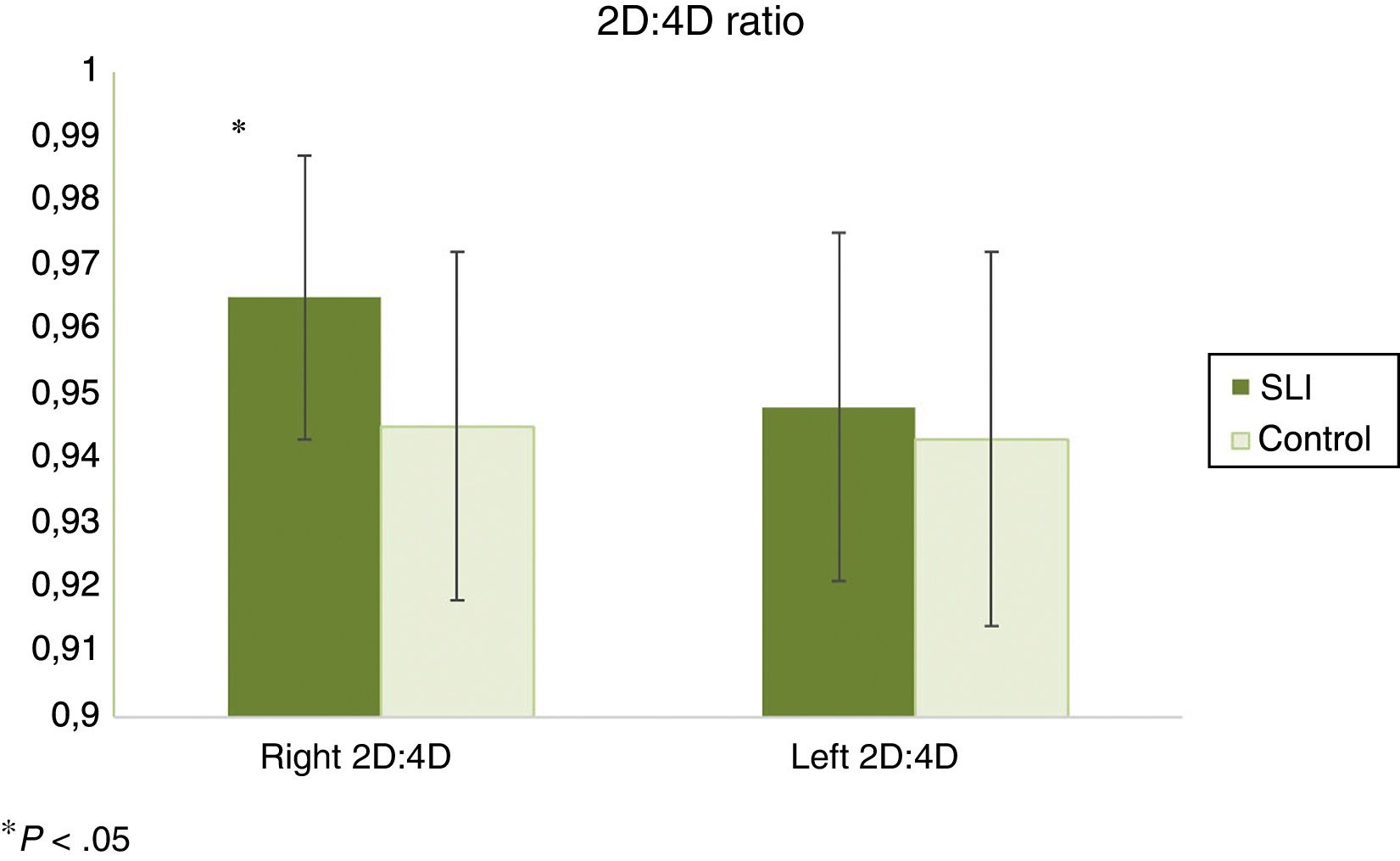
ResultsBiological variablesFig. 1 shows the 2D:4D digit ratios calculated for both hands. We found significantly higher values for the right hand in the group of boys with SLI.

Only 3 boys in the control group and 1 in the SLI group were left-handed. We did not find statistically significant differences in the 2D:4D digit ratio for both hands between left-handed and right-handed boys, nor did we find statistically significant differences in the 2D:4D digit ratio for both hands between the SLI and control groups when looking solely at left-handed boys or solely at right-handed boys.
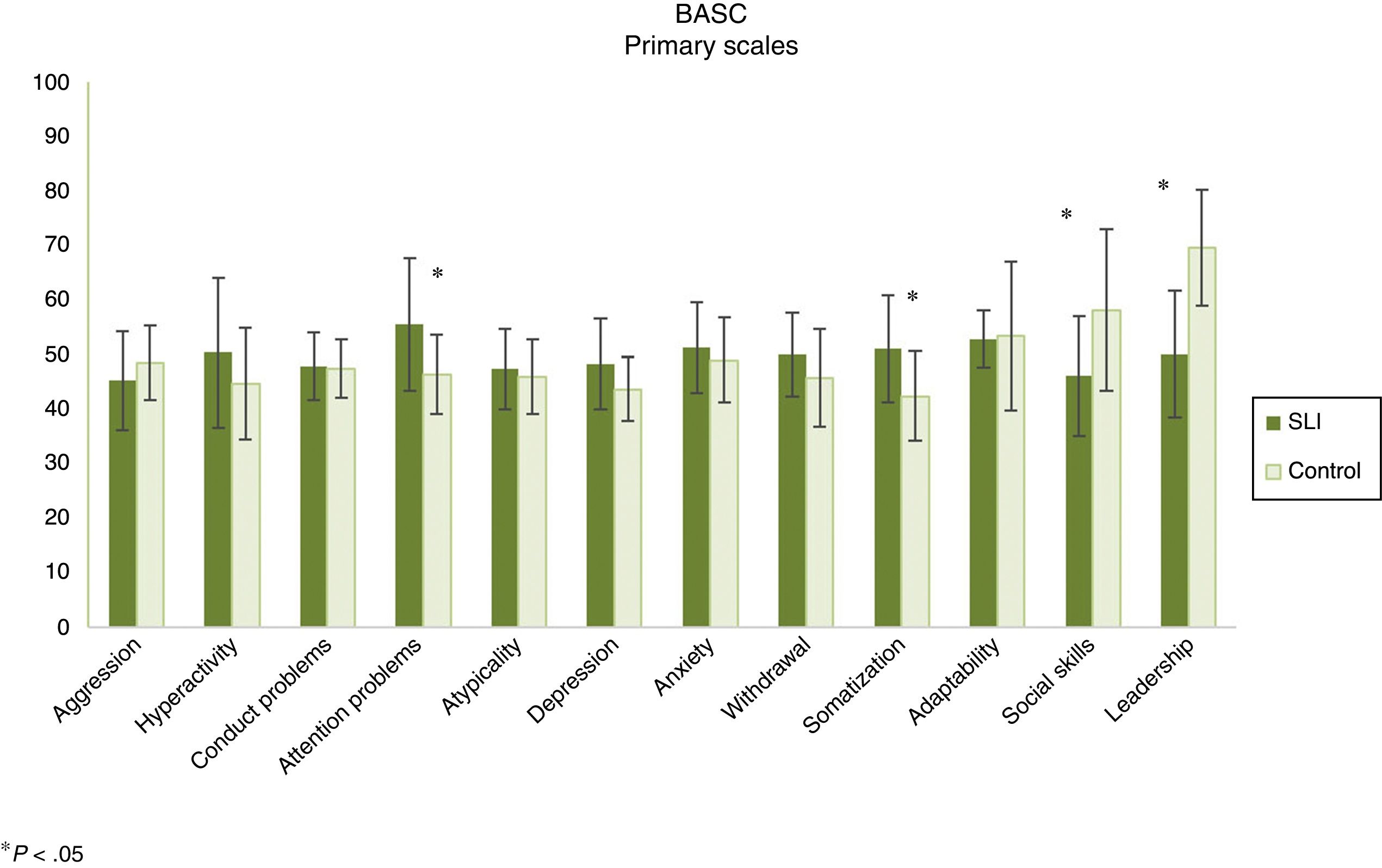
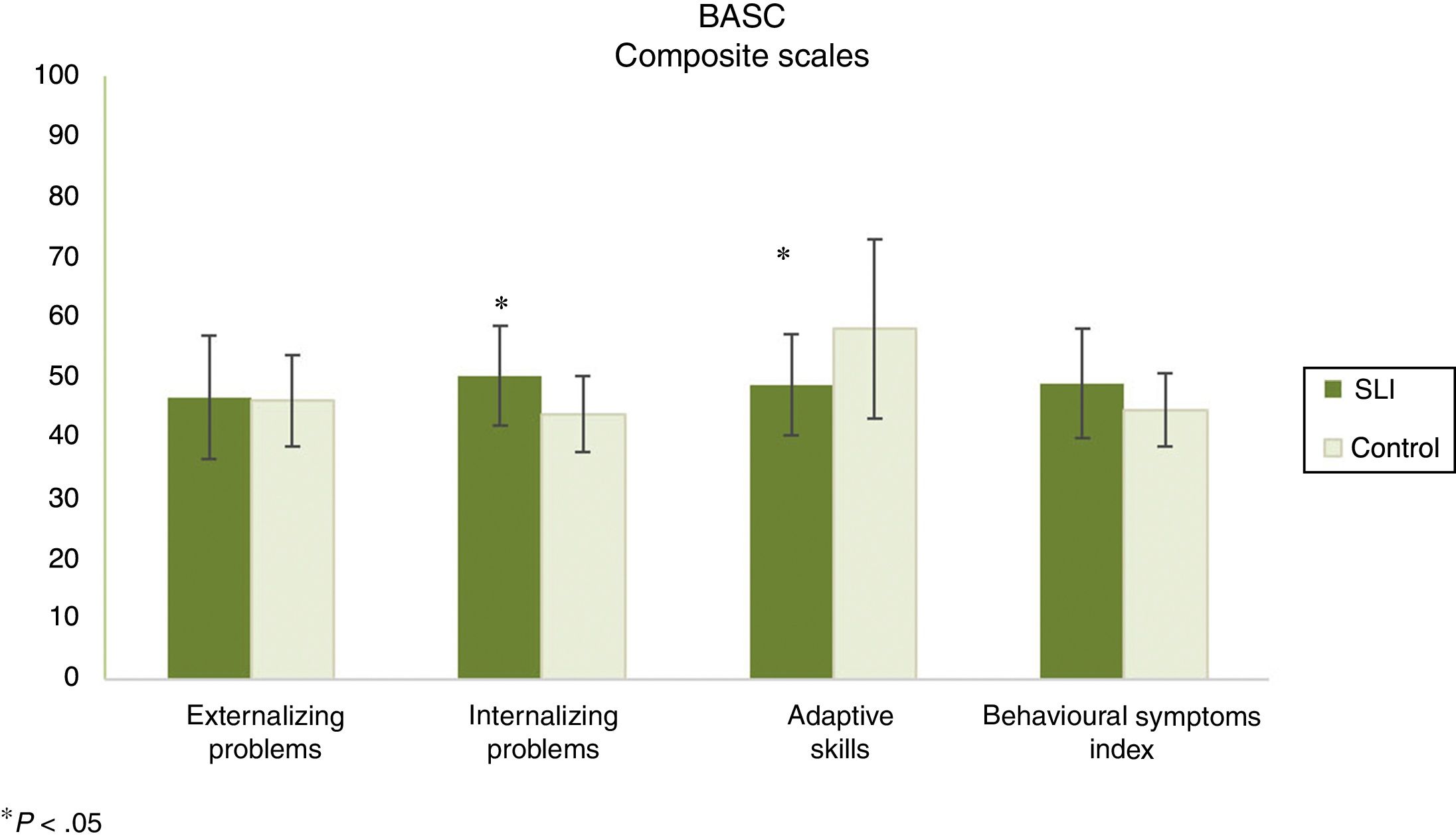
Behavioural variablesWe found statistically significant differences in the BASC scales assessing attention problems, somatization, social skills and leadership, and no differences in the remaining scales (Fig. 2). When it came to the composite scales (Fig. 3), we only found statistically significant differences in the interiorizing problems and adaptive skills scales.


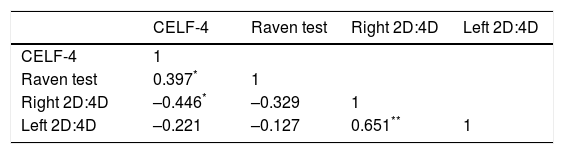
The right-hand 2D:4D ratio was negatively correlated with language skills, but not with intelligence, as can be seen in Table 2. The two biological indices were positively correlated.
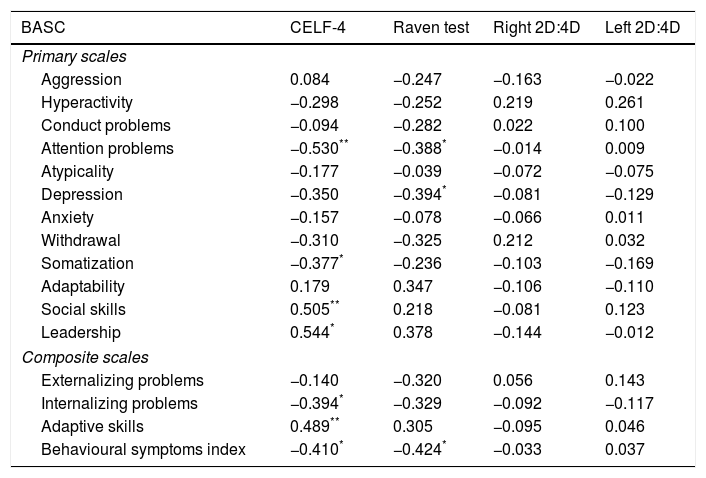
As can be seen in Table 3, the 2D:4D digit ratio was not associated with any of the behavioural variables. However, cognitive and linguistic variables were associated with some behavioural variables. We found that the results in the Raven test were negative correlated with the scores in the behavioural symptoms index composite scale and the attention problems and depression clinical scales of the BASC.
Pearson correlation coefficients (r) for the comparison of linguistic, cognitive and behavioural variables.
| BASC | CELF-4 | Raven test | Right 2D:4D | Left 2D:4D |
|---|---|---|---|---|
| Primary scales | ||||
| Aggression | 0.084 | −0.247 | −0.163 | −0.022 |
| Hyperactivity | −0.298 | −0.252 | 0.219 | 0.261 |
| Conduct problems | −0.094 | −0.282 | 0.022 | 0.100 |
| Attention problems | −0.530** | −0.388* | −0.014 | 0.009 |
| Atypicality | −0.177 | −0.039 | −0.072 | −0.075 |
| Depression | −0.350 | −0.394* | −0.081 | −0.129 |
| Anxiety | −0.157 | −0.078 | −0.066 | 0.011 |
| Withdrawal | −0.310 | −0.325 | 0.212 | 0.032 |
| Somatization | −0.377* | −0.236 | −0.103 | −0.169 |
| Adaptability | 0.179 | 0.347 | −0.106 | −0.110 |
| Social skills | 0.505** | 0.218 | −0.081 | 0.123 |
| Leadership | 0.544* | 0.378 | −0.144 | −0.012 |
| Composite scales | ||||
| Externalizing problems | −0.140 | −0.320 | 0.056 | 0.143 |
| Internalizing problems | −0.394* | −0.329 | −0.092 | −0.117 |
| Adaptive skills | 0.489** | 0.305 | −0.095 | 0.046 |
| Behavioural symptoms index | −0.410* | −0.424* | −0.033 | 0.037 |
When it came to the association between the language assessment measure and behavioural variables, we found a positive correlation between the adaptive skills composite scale of the BASC and language skills. We also found an association of language with the leadership and social skills primary scales that give rise to this composite scale. There was also a correlation, although negative, between language skills and the internalizing problems composite scale, which was confirmed by the negative correlation with the somatization and depression primary scales. Last of all, scores in the behavioural symptoms index composite scale were also negatively correlated with language skills, which was confirmed by the negative correlation with scores in the attention problems primary scale. We did not find an association between any of the assessed language dimensions with the scores in the externalizing problems composite scale or the aggression, hyperactivity or conduct problems primary scales.
DiscussionOur results suggest that it is possible that the language problems of children with SLI are associated with decreased prenatal exposure to testosterone, based on right-hand digit ratio values. We did not find an association with the left-hand digit ratio, which was consistent with previous studies.9,10 Thus, our results contradict the Geschwing-Galaburda hypothesis7 and those of other studies that found a lower 2D:4D digit ratio in individuals (with and without ASD, cognitive impairment or SLI, among others) with poorer language skills (especially in the areas of speech and vocabulary, with no differences in empathizing).9,10,12
In our study, prenatal exposure to lower levels of testosterone was associated with a higher future probability of developing a specific language impairment in the absence of cognitive impairment, especially involving morphology and syntax as opposed to speech and/or vocabulary. Therefore, our results were similar to those reported by Manning et al.14 in that children with language impairment in the absence of cognitive impairment had higher-than-normal digit ratios.
Several previous studies11,13,14 have already evinced the complexity of the association between androgenization and various language and communication problems. For instance, Albores et al.,9 who analyzed the association between the 2D:4D ratio and various measures of language development, did not find a significant correlation between this ratio and language delay. However, they did find a significant correlation between the right-hand 2D:4D digit ratio and speech problems.9 On the other hand, other authors have proposed that the association between prenatal testosterone exposure and language skills may not be linear and may vary between male and female individuals.4 For instance, Burton et al.4 found that men that had been exposed to higher levels of testosterone prenatally (lower 2D:4D ratio) exhibited more severe impairment in language and spatial skills, while women that had been exposed to lower levels of testosterone (higher 2D:4D ratio) exhibited the poorest language and spatial skills. There is also evidence of these complex patterns of association in the clinical population. Thus, Manning et al.14 found a lower 2D:4D digit ratio in children with ASD and cognitive impairment, while children that had ASD without cognitive impairment (or even with above-average intelligence) had greater-than-normal 2D:4D digit ratios.
When it came to behavioural variables, our study also found that, overall, children with SLI have poorer social and leadership skills, more attention problems and a greater tendency to somatise, that is, a greater tendency to internalize problems and poorer adaptive skills, which probably has a negative impact on their social relationships, academic performance and psychological wellbeing. Our results were consistent with those of previous studies.21,22,28,29 For example, Valera-Pozo et al.30 also found significant differences between a group of preadolescents with SLI and another group with normal language development in measures of social skills, leadership and adaptive skills reported by form teachers.
However, based on our findings, boys aged 5–8 years with SLI do not generally tend to be aggressive. Similarly, they show no tendency to exhibit abnormal behaviour or conduct problems. This has also been confirmed by some studies in the literature,20 which have highlighted the absence of aggression as a distinctive behavioural characteristic of children with SLI.
Last of all, our study shows that intrauterine testosterone levels do not seem to have an effect on any behavioural endpoint. However, we did find a correlation between several dimensions of behaviour, the level of language development and the level of intelligence, which suggests that language skills have a greater impact on behaviour than intrauterine testosterone levels. Thus, it appears that behavioural problems in children with SLI are not the result of prenatal androgenization, but rather mediated by their language difficulties. In other words, language problems in children with SLI would result in the development of fewer social relationships and thus on poor development of social skills. This lack of social skills would generate anxiety in anticipation of social interaction, as well as depression, for these children would wish to have relationships but not know how to develop them. In turn, this would lead to internalizing problems (somatization), as difficulties in communication would prevent these children from externalizing these problems. This hypothesis is supported in part by several previous studies with similar characteristics and results.28,30,31
The findings of this study must be interpreted with caution due to a number of limitations: the small sample size, which, while common in this type of study, does limit its conclusions; the fact that we did not have access to a group of girls with SLI and the corresponding control group to compare results with the male sample, and not having collected more detailed information on hormone levels during gestation. Further research on this subject taking into account these limitations would be desirable.
ConclusionsBased on our findings, prenatal exposure to lower levels of testosterone (higher 2D:4D ratio) is associated with a higher risk of developing a specific language impairment in boys. The intrauterine testosterone level does not seem to be associated with the different aspects of social behaviour that are altered in children with SLI (attention problems, depression, somatization, social skills, leadership, internalizing problems and adaptive skills), aspects that, on the other hand, could be explained by the language skills and intelligence level of children with SLI.
Conflicts of interestThe authors have no conflicts of interest to declare.
We thank all the children that participated in the study and their families.
Please cite this article as: Font-Jordà A, Gamundí A, Nicolau Llobera MC, Aguilar-Mediavilla E. Use of the 2D:4D digit ratio as a biological marker of specific language impairment. An Pediatr (Barc). 2018;89:361–368.

