

Over the past 2 years, new guidelines for hypertension in children and adolescents have been published. The first, developed by the 2009 European Hypertension Society Working Group on Hypertension in Children and Adolescents, recognised the need for an update of the European Guidelines in order to incorporate the new information acquired over the last few years. Subsequently, an update of the American guidelines (the most recent of which was in 2004) has been published. In both guidelines, there are aspects which are agreed on, and in others, there are marked differences in the basic elements that have an influence on daily clinical practice. The main differences are centred on the criteria for the diagnosis and classification of hypertension, with the subsequent impact on its prevalence. Future studies should offer responses to all the questions that still remain unresolved.
En los 2 últimos años se han publicado nuevas guías de hipertensión arterial en niños y adolescentes. La primera de ellas, desarrollada por el Grupo de Trabajo de hipertensión arterial en niños y adolescentes de la Sociedad Europea de Hipertensión, recogía la necesidad de una actualización de la Guía Europea de 2009 para incorporar la información adquirida durante los últimos años. Con posterioridad, se ha publicado la actualización de la Guía Americana, cuyo antecedente más reciente se encuentra en 2004. En ambas guías se encuentran aspectos en los que existe acuerdo y otros en los que hay marcadas diferencias en elementos fundamentales que influyen en la práctica clínica diaria. Las principales diferencias se centran en los criterios para el diagnóstico y clasificación de la hipertensión arterial, con el consiguiente impacto en su prevalencia. Ambas guías reconocen y lamentan la falta de evidencia sólida, basada en ensayos para las recomendaciones sobre el diagnóstico y el manejo de la hipertensión arterial pediátrica. Estudios futuros deben ofrecer respuestas a todos los interrogantes que a día de hoy permanecen por resolver.
Advances in the field of high blood pressure, or hypertension (HTN), in children and adolescents have highlighted the need for documents summarising the evidence on the aetiology, assessment, treatment and outcomes of HTN in this age group.1 Our knowledge of blood pressure (BP) in children and adolescents has increased considerably in the past two decades. The first guidelines on the control of BP in this age group were published in 1997,2 as there had previously been no consistent definition of HTN in the paediatric population, and measurement of BP was not performed in asymptomatic children and adolescents.3,4 Although the association between BP and cardiovascular disease is well established in adults, this association in children and adolescents is not well defined, as the development of cardiovascular complications results from the interaction of various risk factors and age. Consequently, the definition of reference values in the paediatric population is based on the percentile distribution of BP values.
Advances in the knowledge of high BP in children and adolescentsThe awareness that HTN may be present in seemingly healthy children and that HTN in adults may have its roots in childhood has spurred interest and demonstrated the need to include measurement of BP in the medical care of children and adolescents. Furthermore, we have gained a deeper understanding of the impact of BP values on the development of subclinical damage in target organs through the use of recently developed methods with a much higher specificity and sensitivity. We are also aware that the prevalence of HTN is increasing as a consequence of the obesity epidemic, which has become a significant public health problem. Early detection of the roots of HTN is crucial for the early implementation of interventions aimed at reducing the elevation of BP and its subsequent impact on cardiovascular morbidity and mortality in adulthood.
Evolution of guidelines for the diagnosis and management of HTNThe current widespread interest in clinical practice guidelines for HTN stems from the desire of health-care professionals to offer, and of patients to receive, the best possible care, that is, care that is consistent, effective and narrows the gap between clinical practice and evidence-based recommendations. The guidelines published throughout the years have significantly expanded the knowledge in this field and stimulated a growing interest not only in epidemiologists, but also in paediatricians and basic researchers.5,6
New guidelines have been published in the past 2 years.7,8 The first ones were developed by the Working Group on Hypertension in Children and Adolescents of the European Society of Hypertension, recognising the need to update the 2009 European guidelines to integrate the evidence gathered over the past few years.6,7 This was followed by the publication of the updated version of the United States guidelines on HTN in the paediatric population,8 which had last been updated in 2004.5
The European and United States guidelines, published 1 year apart, agree on some aspects, but also have marked disagreements on other essential aspects that influence everyday clinical practice.
Agreement between European and United States GuidelinesThe European and the United States guidelines7,8 agree on several aspects, including:
- •
BP screening. BP should be measured starting at age 3 years, and in younger children if they are at risk of developing HTN.
- •
Methods for measurement of BP. The auscultatory method is recommended, using Korotkoff sounds K1 and K5 to assess systolic blood pressure (SBP) and diastolic blood pressure (DBP), respectively. The guidelines also find the use of oscillometric devices validated in the paediatric population acceptable to measure BP.9 However, whenever high BP readings are found by the oscillometric method, the auscultatory method must be used for confirmation.
- •
24-h ambulatory BP monitoring (ABPM). It is considered useful both for diagnosis of HTN and to monitor pharmacological treatment.
- •
Treatment. Once HTN is diagnosed, both guidelines agree that lifestyle changes should be introduced and BP rechecked repeatedly, initiating pharmacological treatment if these measures do not achieve adequate control. In cases where the elevation of BP is such that it poses a risk of organ damage, pharmacological treatment should be initiated immediately.
The main methodological differences involve the criteria for diagnosis and classification of HTN. This is due to: (a) differences in reference values; (b) difference in the age used to apply the adult criteria for definition of HTN, replacing the traditional approximation by BP percentiles and (c) differences in the classification of HTN.
- a)
The reference values for BP come from the same source in both guidelines, the 2004 US Task Force cohort.5 While the European guidelines maintain the percentiles of the original cohort, the United States guidelines calculate the percentiles based only on children with normal weight. The exclusion of children with overweight or obesity, which were included in the original cohort, was founded on the risk of bias that could lead to underdiagnosis of HTN.
- b)
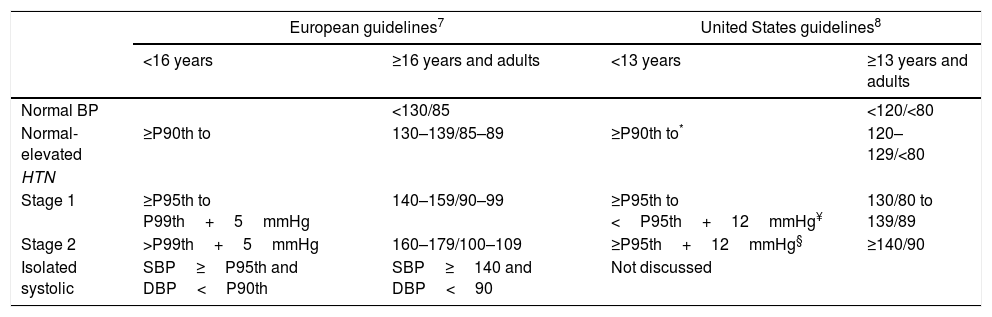
For the diagnosis of HTN, both guidelines use BP percentiles for age, sex and height, until the age of 16 years in the European guidelines and the age of 13 years in the United States guidelines. Starting from these ages, adult criteria are applied to define HTN: 140/90mmHg in the European guidelines10 and 130/80mmHg in the United States guidelines,11 thresholds that are not free from controversy (Table 1).12,13
Table 1.Definition of normal BP and HTN in children and adults.
European guidelines7 United States guidelines8 <16 years ≥16 years and adults <13 years ≥13 years and adults Normal BP <130/85 <120/<80 Normal-elevated ≥P90th to 130–139/85–89 ≥P90th to* 120–129/<80 HTN Stage 1 ≥P95th to P99th+5mmHg 140–159/90–99 ≥P95th to <P95th+12mmHg¥ 130/80 to 139/89 Stage 2 >P99th+5mmHg 160–179/100–109 ≥P95th+12mmHg§ ≥140/90 Isolated systolic SBP≥P95th and DBP<P90th SBP≥140 and DBP<90 Not discussed P90th, 90th percentile; P95th, 95th percentile; P99th, 99th percentile.
* or 120/80, whichever is lowest.
¥ or 130/80 and 139/89, whichever is lowest.
§ or 140/90, whichever is lowest.
- c)
The definitions of stages 1 and 2 also differ between the European and the United States guidelines, as the latter applies the criteria of the published guidelines for the adult population (Table 1).7,8
The choice of age 16 years in the European guidelines is based on the fact that in adolescents aged 16 and 17 years, with the exception of males aged 17 years at or above the 95th percentile for height, all the specific values for the 95th percentile for BP are below the threshold used to define HTN in adults. When adolescents become adults, this difference may lead to an adolescent previously considered to have HTN to be considered a normotensive adult on turning 18 years old due to discrepancies in definition criteria.
The United States guidelines lower the age for application of adult BP criteria to 13 years. It could be argued that simplifying this criterion for the diagnosis of HTN would facilitate the identification of children at higher risk of cardiovascular disease. When the threshold of 130mmHg is applied at the age of 13 years, it is below the 95th percentile for age, sex and height in male adolescents, whereas the opposite is true of female adolescents, in whom the 95th percentile does not reach 130mmHg in any instance.
Impact on diagnosis and treatmentThe first consequence of these differences involves the prevalence of HTN. The United States guidelines result in a greater proportion of children considered to have HTN, although not in a greater proportion needing pharmacological treatment.
This greater prevalence leads to increases in:
- a)
The patients requiring clinical monitoring.
- b)
The use of 24-h ABPM, due to the recommendation that “ABPM should be performed for the confirmation of HTN in children and adolescents with office BP measurements in the elevated BP category for 1 year or more or with stage 1 HTN over 3 clinic visits (Grade C, moderate recommendation).”8 Both guidelines7,8 recognise the usefulness of ABPM for the identification of white-coat HTN and masked HTN and that it is the sole method available for diagnosis of nocturnal HTN, which carries risks that are independent of the daytime ambulatory and office BP values. The reported frequency of white-coat and masked HTN varies as a result of the office and ambulatory BP criteria used to establish the diagnosis. In this context, the lower office BP values established by the United States guidelines for the definition of HTN will result in a marked increase in the proportion of individuals with white-coat HTN, as the reference used to define HTN by the ABPM method continues to be the distribution tables obtained for the European population.14
- c)
Performance of diagnostic tests to assess early organ damage. The timing of the evaluation of potential target organ damage has considerable clinical relevance. The assessment of left ventricular mass continues to be the key in the investigation of early signs of organ damage. Children and adolescents with HTN may have left ventricular hypertrophy even in the early stages of disease,7,8 and delaying evaluation may lead to errors in risk stratification. The European guidelines recommend monitoring target organ damage after HTN is diagnosed and considers its presence as an indication for initiating pharmacological treatment; the United States guidelines recommend assessment of left ventricular mass only at the time that pharmacological treatment is considered. Thus, the European guidelines promote the assessment and detection of target organ damage as a way to establish the need of pharmacological treatment in children and adolescents with HTN.
- d)
The ongoing debate on the BP targets to pursue in treatment is also considered in the recommendations of both guidelines. In children, the evidence supporting specific BP targets is scarce, and there is also uncertainty regarding the specific impact of drugs on cardiovascular and renal outcomes. In the absence of prospective, long-term studies on the impact of different BP levels in intermediate or final cardiovascular or renal goals, the 95th percentile is considered the BP target, as this was the threshold used to define HTN in children and adolescents, although lowering BP below the 90th percentile would be preferable as long as the treatment is well tolerated. In individuals aged 16 years or more, the European guidelines recommend establishing targets using the cutoff for clinically significant BP in adults, that is, of less than 140/90mmHg, without discouraging the goal of less than 130/80mmHg. Conversely, the United States guidelines recommend reducing BP to less than 130/80mmHg starting at the age of 13 years.
- e)
When it comes to patients with chronic kidney disease (CKD), the European guidelines recommend a BP target below the 75th percentile in children with nonproteinuric renal disease and a BP target below the 50th percentile in those with proteinuric disease.15 This recommendation differs from the United States guidelines, which recommend a BP target below the 50th percentile in nonproteinuric patients, too, although there is no evidence that this measure provides additional protection against renal events in nonproteinuric CKD.16
Finally, isolated systolic HTN, the most frequent type of HTN in adolescents, has been specifically considered by the European guidelines7 (Table 1) but not the United States guidelines.8 In a high proportion of cases, elevation of SBP with a normal DBP is associated with normal BP in the aortic root. Various mechanisms may be involved in these discrepancies, but this phenomenon nevertheless affects clinical decision-making. At present, we accept the recommendation that patients with isolated systolic HTN undergo measurement of central aortic BP by indirect, non-invasive methods, as this allows the detection of left ventricular mass abnormalities. In patients with normal central BP and left ventricular mass, it is possible to apply a watchful waiting approach without initiating treatment.17
Future needsAll published guidelines acknowledge and lament the lack of robust evidence from clinical trials on which to base the recommendations for the diagnosis and management of paediatric HTN. To fill this gap, action must be taken to gather data that will result in relevant evidence in upcoming years. To determine the usefulness and appropriateness of the new BP threshold, future studies ought to analyse the effects, both in the short and the long term. The long-term analysis involves the challenge of assessing the incidence of cardiovascular complications of HTN over many years. On the other hand, in the short term, we need to explore new strategies for improving control of BP without significantly increasing the cost, work burden and side effects of treatment. Future studies must attempt to answer all the questions that remain unresolved to date.
Conflicts of interestThe author has no conflict of interest to declare.
Please cite this article as: Lurbe i Ferrer E, La hipertensión arterial en niños y adolescentes a examen: implicaciones clínicas de las diferencias entre la Guía Europea y la Americana. Ann Pediatr (Barc). 2018;89:256.

